
Yesterday afternoon I received the anticipated phone call from Nancy, RN, at the Stephenson Cancer Center with some enlightening information about the results of my bone marrow biopsy from 25 February. It has led me to do a little more research into my condition, which is admittedly a very confusing and complicated cancer to understand and explain.
I am including a link to an article from the International Myeloma Foundation’s website that explains the different types and subtypes of Multiple Myeloma. Reading this stuff reminds me of understanding Algebra back in the day when I was in high school. I understood it in moments of clarity that would come and go like a strobe light. Numbers have never been my forte; I’m a word girl. I know when I’m looking at my lab results where my focus is, but after this most recent biopsy, I realize my focus has been too narrow.
Within our marrow there are several types of white blood cells. They make up the majority of our immune system. Certain white blood cells called plasma cells secrete large volumes of immunoglobulins as antibodies to fight infections. Immunoglobulins are proteins that attach to substances entering the body that the body recognizes as foreign. Normal immunoglobulins are called “polyclonal protein.” Myeloma cells, which are cancerous plasma cells, secrete monoclonal protein, which is an abnormal immunoglobulin that cannot properly fight infection. The immunoglobulins are abbreviated “Ig.”
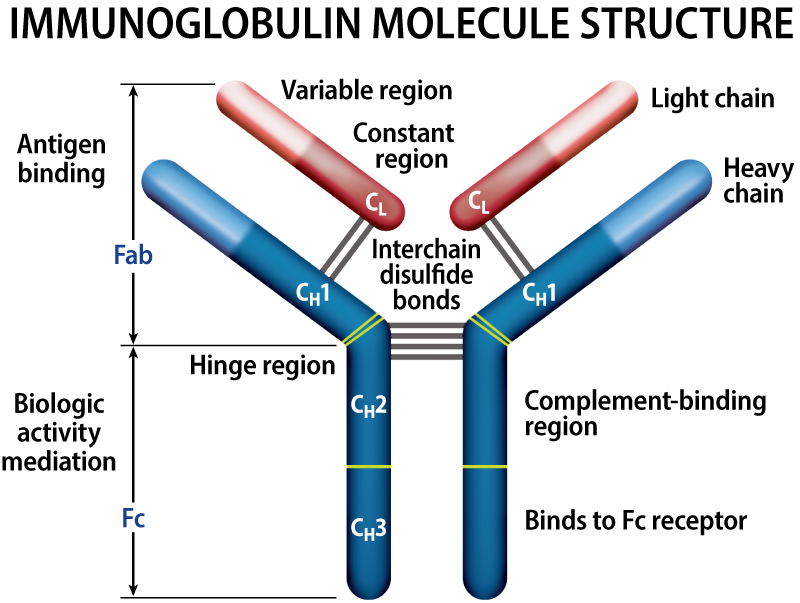
On a molecular level, these immunoglobulins are made up of two heavy chains and two light chains that are bound together. There are five possible types of heavy chain immunoglobulins, and they are, from most common to least common: IgG, IgA, IgE, and IgM.
There are two possible light chains: kappa and lambda.
With myeloma, the immunoglobulins make up only one type of heavy chain, in my case A, and one type of light chain, in my case kappa. So, in my plasma, there are two IgA heavy chains bound to two kappa light chains. Because they are monoclonal, some of the problems they cause are the tumors, or lesions, that were found on my bones that essentially are holes or weak spots. These showed up as illuminated areas in my PET scan. Left untreated, these abnormal immunoglobulins can lead to more bone damage and eventually kidney failure.
In my phone call with Dr. Joudeh on Tuesday, he mentioned a 10% figure that represents the concentration of these abnormal cells in my bone marrow. Nancy told me that this is not a bad number, but rather, since I will not be doing the transplant until May, we have time to get it to a more optimum number of around 5%. The lower the number, the better the chances that the transplant will be successful.
One of the questions I asked Nancy was why Dr. Selby decided I should be given a new chemotherapy drug, Darzalex (daratumumab), when I had a cycle of Revlimid in hand that I could take. She said he felt there was a greater chance of attaining the 5% goal with a change in chemotherapy, considering that after four cycles of RVD (Revlimid/Velcade/Dexamethasone) I had not been able to get there.
“Cancer cells are tricky,” she said. “They can adjust to chemo drugs so that they become less effective over time.” I recalled the conversation with Michelle, the owner of A Wig Boutique in Pensacola who had told me about how her Hodgkin’s Lymphoma had stopped responding to the chemotherapy, and that is why she had to have a bone marrow transplant.
As I was writing this post, I got a call from one of the infusion nurses at The Woodlands. The Darzalex has been approved by my insurance, and my first infusion will be on Monday. It will take 8 hours.
“Can you be here at 8 a.m.?” she asked me. I told her I could and asked if I could bring my laptop.
“You can bring your laptop, a pillow, a blanket, some lunch…whatever you like. You’ll be in a room in the back where you can use your computer or rest or whatever you feel like doing.” She told me in addition to getting the Darzalex intravenously, I will also receive my regular Velcade injection.
She explained that Dr. Joudeh would do a teaching session with me tomorrow for the new therapy so I will know what to expect. I’ve already read about possible side effects, which are comparable to Revlimid and which I hope will be mild. According to the Darzalex website, for patients like me, the drug is used “in combination with the medicines bortezomib (Velcade) and dexamethasone in people who have received at least one prior medicine to treat multiple myeloma.”
I hope some of you will text me or send me a message on the blog! I would love to chat during Monday's first marathon session.
References:
International Myeloma Foundation. https://www.myeloma.org/types-of-myeloma
I had written a note but of course, I messed up and it didn't go thru. Surprise, Surprise! I will try again. I wanted to tell you that the elders of our church pray for each family as much as possible and on a personal level. We got a call this past Wednesday morning telling us the eldership would be lifting us up in prayer that night and if there was anything special we needed them to pray for. I asked for prayers for you, the new treatments, for your peace and comfort and for your boys. "I always call them boys even though they are men now!" I asked them to pray the boys are able to be clos…
Thanks for this entry Kelly. I really appreciate you taking the time to share so much information. Wishing you the best on Monday and will put a reminder in to check in on you. So thankful that the “insurance gods” got the approval this soon. That has got to add some to the anxiety opportunities waiting on those decisions!
blessings!